Jerry_Atrick
-
Posts
960 -
Joined
-
Last visited
-
Days Won
3
Content Type
Profiles
Forums
Gallery
Downloads
Blogs
Events
Store
Aircraft
Resources
Tutorials
Articles
Classifieds
Movies
Books
Community Map
Quizzes
Videos Directory
Everything posted by Jerry_Atrick
-
 I think this sums it up...
I think this sums it up... -
When people trend to be losing the logical side of the argument, they resort to mockery and other forms of baseless ridicule or irrelevance to try and affect the debate. Remember Trump in his initiak days? How many Journos did he call a "bad, bad person" without actually answering the questions of providing credible facts? He does it today. We all mock trump for this, but some people exhibit the same tendencies. As I mentioned, point us to the credible evidence that suggests otherwise - until then - I would suggest it is those who can't that are not willing to see reason or change their mind..
-
Any Cardinal Pilots out there?
Jerry_Atrick replied to KRviator's topic in AUS/NZ General Discussion
A mate of mine, originally from Toowoomba, has one - G-ZION (google it - you will see photos of it and if you google G-INFO (CAA's aircraft database), you can check out all the details. It is a 180HP model, fixed undercarriage, 1972. I've been in it a couple of times and it is a good machine. EJB looks to be a retractable; G-ON is fixed gear from memory.. Apart from that they should be more or less the same with a slightly different useable load. While you're not going to need a g-suit, they are no slouch for the type of aircraft they are. They have a bigger cabin than the C172 and people thought they could just stuff the cabin full like they could the 172... big mistake. The numbers look OK to me, but I am sure a little googling will work it out for you - are there any STCs on it? Avweb had a good article on them: Cessna 177 Cardinal I would certainly look at a later model... Mate's aircraft is here: Cessna 177B Cardinal, G-ZION / 177-01690, Private :. This was before he owned it. As with any used aircraft (ir any used mechanical item), you are buying what the previous owners did and did not do in terms of mainternance, and in the case of aircraft, g-forces. On the first annual, the exhaust had to be replaced and a few other wearable items.. so far, as far as I know, nothing major (well, beyond a few thousand £). -
Agreed OME... it is getting heated... And it really just goes in circles. But since what was a light-hearted joke about those in Vic (Mexico) making it across any border by air since the re-lockdown has since morphed into [yet another] debate about the appropriateness of the lockdown. There is little to do with aviation so maybe mods should consider locking down this thread and transferring it to socialaustralia.com.au? I have noticed traffic there is really light lately... That said, I'll bite... The main arguments against the lockdown seem to be: It only affects the aged and those with co-morbid conditions. Not entirely true. There were young people with no identfied (after autopsy) co-morbid conditions.. these are reasonably rare, but tell that to the families of the victims. Of course, I agree we shouldn't put the world on hold for that alone. For the aged care facilities - they were in lock down but the infection still spread from carers; And being in an aged care facilitiy doesn't mean you're going to drop dead in a short time.. My stepfather was in one for about three years; my partner's grandmother was in one for about two.. There were many in these facilties that were there longer. Finally, co-morbid does not meen a condition that is life threatening nor life shortening. It simply means, " relating to or denoting a medical condition that co-occurs with another", or from wikipedia: " comorbidity is the presence of one or more additional conditions often co-occurring with a primary condition. " Bronchopneumonia is commonly cured - yes people die from it.. Many respiratory and other organ conditions may be chronic but not materially life shortening. I get the feeling to some people co-morbitiy means another condition that threatens or shortens life.. Also, wikipedia is not the deifnitive, but it states that co-morbitiy is not the primary condition.. Someone posted an April BBC article reporting the risk of COVID and the fact that they report a COVID death even if the co-morbid condition is the primary cause. It then went on to say that the primary cause is in the majority was COVID... And what it didn't say is that the numbers are adjusted up to 3 days later to cover late reports and corrections to the cause. Only a small amount of the population get it, and it is only fatal in a small percentage. Well, I would agree, especially in Australia, only a small percentage get COVID. But this will mainly be because Australia went comparatively hard and fast saving a situation like that which played out in the US or the UK. This should give you a view of the current numbers in the US. We can see almosy 1.5% of the populaton have contracted it so far, and that almost 3.3% of those have died. Compare that to Australia, where you have 0.08 percent of the population and the fatality rate is up to 1.24%. The US is more densly populated, but US cities in sq miles are as large as ours and over 60% of the Aussie population are reside in the state capital cities so there is ample desnity for the virus to spread in our popualtion centres.. especially since entry into the country is probably 99.9% at these cities. The point is the US had at best patchy controls, Australia was a lot better... The stats speak for themselves. And of course, Aussies knew the healing properties of dunny paper.. Of yeah, look at the graph on the Aussie chart.. from a very small number of cases, a very quick increase in the daily rate..This would indicate the exponential infection rate (a curve would be shown on cumulative numbers). This shows the rate at which it will spread ifg ledt in mild check... Note, the US hosptial system couldn't deal with the crisis.. that may be a good indicator as to why their fatality rate is almost three times ours... And their infection rate is what times ours? Thousands of people die per year from influenza, but we don't take these sorts of precautions: Yes, this is true. According to the WHO, up to 650,000 per year die from respiratry complications associated with the flu (so that is quite a lot more than those atrtrubuted directly to the flu, and this should atone for the co-morbitiy issue with COVD deaths). If you look at the Australia and the US charts above, you will see that globally we have exceed 692,000 deaths and this is only 8 months old.. Also, this doesn't include deaths from subsequent complications brought on by the disease. I think on all counts, it has already exceeded the death count with the flu... It won't be long until the flu has a bit to do to catchup. I looked up fatality rates for influenza and got a lot of sites that were convoluted, so couldn't be bothered to crystalise the numbers to get a comparison. But, note, there is no coordinated effort (other than a voluntary flu jab) to contain the flu; there is one for COVID. So numbers not quite like for like. The numbers for COVID-19 appear to bear a rather grim projection should some serious action not be taken. This is an overreaction that will wreck the economy. This is a prediction, and there is probably some evidence we can draw from the previous SARS epidemic and maybe even the Spanish Flu (incidentally which did not originate in Spain, but was the worst affected as they didn't implement the lockdown measures of the day). The UK is talking about a V-shaped recovery - i.e. quick to decline, but quick to recover. This article from a couple of weeks ago talks to it.. However, there is concern it won't be V shaped.. I agree.. it will be a shallower curve on the upside because people are tentative and jobs have been lost, companies will have closed, etc. People (in the UK) don't frequent pubs, cafes, etc at anywhere near the rate the did pre-COVID. This month, the UK government will foot 1/2 the bill of all in-restaurant/cafe/pub meals.. and so far no one I know has taken up the offer. People will spend less while the virus is perceived to the a threat. They will not go out as much, etc. The longer the threat, the slower will be a recovery. Also, the more people who die, the more of the economy you lose (except for funeral directors and cemetries/crematoriums). Yes, there is public borrowing that will have to be paid back. yes there are SMEs that will close their doors forever (mine is probably one of those). But at the other end of it, new SMEs will grow (hopefully a new one for me), the government issued debt is the cheapest you can get at the moment, and allowing the virus to persist will keep economic activity suppressed and require higher borrowing and more SME failures than there should be and recovery will take a lot longer. etc. The collateral damage (e.g. mental health) will be much higher than the lives it saves: This one has merit.. but as we don't know how many lives are being saved by the lockdown versus how much more collateral damage is happening, it is very hard to make a true judgement. The main concerns I hear of are mental health deteriorration leading to suicide, and the fact that there are much lower rates of cancer diagnosis meaning many cancers may go undetected that can be saved. This is a real issue where to be honest, a balance has to be found and the lack of numbers that can be causal make it difficult to assess. However, should COVD rates increase, even without a complete rip through the community, there will undoubtedly be a lot of mental anguish and possible suicides as a result. Also, the ability to treat other medical conditions will be severly affected because COVID wil ltake up so much medical resources.. so I am on the fence on this one in the absence of data Each state is doing their own thing: Yep - I get it.. that is the law of the country (and that of the UK, too). And I agree with it.. It is compeltely stuffed to have different, albeit similar approaches for the one country (or in the case of the UK and Europe, I would even say one land mass) as no virus really gives a toss about artifical borders put up by man. Also, it is whacky that I can't go to either side of a line on a map based solely on there being a line, despite all the factors being nearly identical across the line and there being no additional risk... It is nuts.. but that does not say the measures being taken shouldn't be being taken... Yep.. they should at least be coordinated and consistent. Also, if it were Australia wide, we have to accept that in areas there is a breakout (such as Melbourne and now Sydney looks like it has a cluster), then localised lockdowns under a Federal response would be appropriate, would it not? Duing lockdown, we should be able to go flying: If we have our own plane at our own or a local airstrip (say within a 5km radius) and we go flying ourselves or with someone in the immediate household, yes I agree. But as Turbs pointed out, there are too many rec activities that may or may not fall into the safe category, naming all those that are allowed or those that are not (and for certain activities the conditions under which they are or are not) is just not practical. And as we have seen, too many will try it on if they think they can. Even in the case of flying, say you are within 5k of Moorabbin.. and you want to rent a plane from RVAC? Probably shouldn't allow that because the risk of contact will be too high.. Now what about going to Redcliffe or some other country airport with a moderate amount of activity, or even low, but shared (e.g. rentals, syndicates, etc). You can see the line gets blurred and it is very difficult to enforce. Yes, the state government has allowed fishing (maintaining social distancing) and some other things.. can't recall.. Maybe Dan likes fishing.. or maybe they have looked at what the majority of people do. I understand the frustration of being needlessly grounded.. I know folks outside of Melbourne can probably go flying... but this was a real issue day 1 or the original lockdown. Multiculturism is increasing the spread because they won't comply: If this is the case, it still doesn't stop the requirement for the lockdown and it is an error to conflate the two. Anyway, I understand there are those of different religious and cultural backgrounds have been breaching lockdown. However, there are also a lot of caucasion Aussies doing it, too. Bunnings' Karen, the couple who drove to Orbost or wherever and were infected; and the infamous Wodonga Burger Run... - Seriously? From the above, I think a natural human trait is not to be kept isolated and try it on... BTW, if you are taking your news from Sky or other "right wing" press, maybe you want to watch in full about the Melbourne based South Sudanese treatment by the such press here: https://www.youtube.com/watch?v=5ZCfpvP1TSg:367 Other miscellaneous topics: The three main ones are.. "for the mathematically illiterate..", "... well said"., and something like they'll never listen and won't change their mind. Well. I think the above prose (of which I have spent too much time on to be honest) shows that at least I listen to the arguments - both sides! My mind hasn't been changed because I like to back up opinion (or more accurately, intuition) with facts in these cases. There is no one absolute right way to handle this... There isn't really a precedent in Australia nor most of the developed world in handling this in modern times. So, it has to be a balancing act - and a difficult one at that. However, from all the data the countries who are taking the harder line are medically and economically recovering faster than those who aren't. As for the "mathematically illiterate", let me know which statistical technique you would like. Hist Sims will be difficult, We could use tobit or Beta -logit probability methods;' monte-carlo simulations (path or non-path dependent), even Bayes Theorem if you like... probably path dependent monte carlo or Bayes is the most applicable. But the simple ratios and maths are already illuminating. Now, I would never attempt these moreadvanced techniques with medical data as I have no idea of the data issues/smoothing techniques, bias, etc. But that is what the professional modellers do and while I can guarantee they won't get it 100% right, so far the comaprison between countries points to them getting it largely right (which any statistical method is about, which is why VCE maths for a while changed from pure and applied to change and approximation). And we certainly don't rely on questionable sources of statistical analysis against government (or in some of the above, wikipedia - which is not so reputable but at least can be corrected). Yes, we could isolate oldies (of which a few of us are on here, which would mean no flying) and those with known co-morbid conditions. This may slow the fatality rate, but it ignores that even that isolation requires some form of interaction, that the virus will still continue to spread, herd immunity is not provem, there will be spillover into quarantine, people will shun Aus because they don't want to get it because it will still be in the community with Aus, we won't go out as much or do the discretionary things as much because we don't want to tempt fate, etc. Sorry fellas, at this stage, you haven't convinced me it is a good idea not to go for lockdowns and eradication or live with hard lockdowns for clusters as they form.. yet.. Of course, an anti-viral inhibitor or decent viral vaccination may change that... Give us good evidence and you will at least change my mind. Of course, with reputable data to show the medical and economic effects won't be worse inthe long run will change my mind, too.
-
Agree 110%.. My point though, was if one is going ot buy - then buy locally and better still from clearprop as it helps keep the forum going
-
Are these not just as good? CO Detector. Should be less than the total price per unit fom the US (inc. postage).
-
I am sure there is nothing to worry about, but wishing him a speedy recovery...
-
Blimey! I hope there is enough dunny paper in Vic
-
Great shots, Mr. Jessup. I try not to read the location before I look at the shots and thought it was Lakes Entrance... Hasn't changed much from the air. All very green given it was burned out not too long ago. The south east coast and around up tpo Bermagui (as far as I have been in a light aircraft frrom Moorabbin along that route) is almost gods country...
-
Yes he has... because he doesn't want it to get to a state where the hospitals and health care facilities can't cope.. and if you live outside Victoria, guess what.. .neither will you as they will lilekly ship Covid patients to other states' facilities that can take up the slack. It is, after all, one country, isn't it? The state's health system is sized based on expected demand plus a decent amount of fat for contingencies, etc. There is not pot at tghe end of the rainbow that has a never ending supply of staff, hospitals or the equipment that goes into it. I agree it is draconian.. .I agree I would never thought I would live to see the day a massive curfew in any city in Australia would be subject to it. Unfortunately, a small minority of people decided to not comply with the looser restrictions that would in all probability have not required this to occur... You have seen from the stats how a small number of community transmissions can quickly balloon out. We can see stats from around the world that as the cases mount and the health facilities come under strain, the rate of fatalities per infections escalate (as the stats state, Aus, 1.07%, US, north of 3.5% - more than three times ours because it blew out the health system). If you want to know how people will look back and judge this.. Let's look at the UK, which went slow and has one of the worst fatality rates per 100k population: Since mid-April, his popularity rating has plummeted. The press and every day people, who were very supportive of him initially are highly critical saying he didn't go fast and hard enough to start with (admittedly, he was acting on the advice of the CMO). Further lockdown easing was delayed on Friday by two weeks and with it came a stern warning that increases in infections will result in tighter restrictions.. After this week, where we had some great weather and people flocked to the beaches and largely ignored social distaincing, two weeke hence should start showing whether or not this is a hoax.
-
Country Airstrip Guide NSW Download
Jerry_Atrick replied to Aussie Aviation's topic in AUS/NZ General Discussion
I think it should be allowed to be updated as a historical record. As pilots we should be verifying the recency af any planning data we use, correct? -
Country Airstrip Guide NSW Download
Jerry_Atrick replied to Aussie Aviation's topic in AUS/NZ General Discussion
It seems to be on their site... and they are not asking any money. Also it is a 2003 edition... -
And you point is? The reason why it is still statisically low is the measures taken.. The compounding an exponential effect will see the cases rise pretty quickly if things were allowed to continue.. And when one runs out of medical facilities to treat, not only are the absolute amount of deaths gong to rise, but so too is the fatality rate of those infected. This is not a linear relationship (for us mathematically illiterate). Earlier this week, the Aussie fatality rate was 1.07% of those infected; in the US it was well over 3%... Yeah.. double f all is f all, but doubling the doubling the doubling.. well you get the idea.
-
Wait 2 years when the GTX2080Ti is superseded... the costs will remarkably come down and they will still be making a profit...
-
So do you know the answer - 50 tons of Canaries
Jerry_Atrick replied to SSCBD's topic in AUS/NZ General Discussion
They never shut up (they aren't that far from us)... -
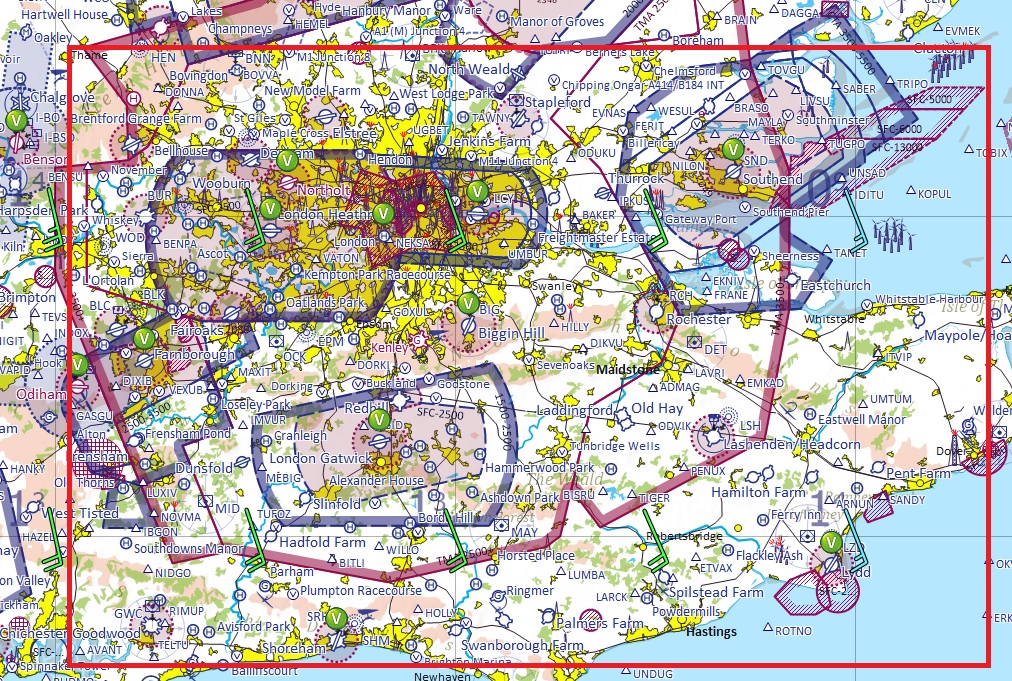
Many seasoned pilots make mistakes.. Radio is not perfect - just another weapon in the safety arsenal. The area in the red square (Willedo should like that) is probably the busiest GA airspace in the world on a good summer's day because it is where highest conecntration of GA/rec planes are based or pass through, it is full of no-go controlled airspace, particularly the Heathrow CTA (which is as low as 2,500' for long distances), Heathrow CTR, London City, Gatwick, Luton, Stansted, Southhampton, a couple of yearrs ago, Southend and now Farnborough all have Class D CTRs. So, most airgraft, GA and Rec, fly around the squeezing many aircraft in a small area and it does get very tight. Farnborough operate 3 LARS services (West, North and East) that roughly cover the box, with assitance from RAF Benson when it is active. Although some pilots are "purists" and would not entertain even carrying a portable in their vintage or grass-roots planes, there is no way in hell I would go there withough a radio. It gets so busy (with the ridiculously long calls we have to make), that last time I flew I couldn't get a word in edgeways. But we now have listening squawk codes; so we set the transponder to that ATC unit's listensing code and they know we are (supposed to be) on frequency and will call us if they feel we need to. Works pretty well. A couple of times while on a listening squawk I have been warned of conflicting traffic that I could not see. When we leave the area (or in my case, switch to the aerodrome information frequency), we squawk 7000 (general VFR code and a reason why they never issue a code ending in 500, 600 or 700). Where the airfield we are arriving at is within an airport CTR, the airfield will have an agreed squawk code so the airport ATC know that the aircraft is entering the CTR for that airfield.

-
Could it be that one was not on the right frequency?
-
Or, as happened with me, a pilot announced he was entering the airfield ATZ (airfield traffic zone - UK) when he was actiually entering downwind and we only saw him emerging from the sun literally with moments to spare. I filed and airprox on that one. If I am overflying an airfield ATZ, (std dimensions are 2.5nm from centreline of the longest runway if more than one and 2,000' AGL) I will call them up to let them know what I am doing if I am flying less than about 1,500' above the ATZ height. But, for airfields without one, I won't generally call them up. Usually most aircraft enroute are not at or below circuit height - I never am (but it does happen)... So, in answer to your question, I would (not knowing CASA advice/regs) start onairfield frequency and shortly after leaving the circuit (with no ATZ active) would switch to area.. Any incoming that would present an immediate risk should have been on the frequency and announced themselves by that stage. Even with an ATZ active but no radio (which does occasionally happen - in which case you need prior permission), I wouldprobably witch to area frequency shortly after leaving the circuit. Having a radio is no guarantee of safety.. Nothing we have available is a guarantee of safety (not even TCAS)... But they are part of the weaponry in our arsenal to help reduce the risk and improve safety.. Our eyes aren't going to guarantee us safety, either, but we don't fly around with our eyes closed... (Yenn, I am not having a go at you as you didn't say no need for a radio - just making sure anyone who is inexperienced reading this doesn't think to themselves they should dispense with one). In GA aircraft, it is typical of club aircraft at least and many private aircraft to have two radios. You can had 1 set set as the communication set - so listening and talking to your local airfield frequency and the other set to listed to the area frequency. I know for recreational aircraft this is typically not the case (at least over here), but I would rather one than none. Evenin remote areas where thereis no ATC coverage, if your donk quits, you may be picked up transmitting your mayday by a passing airliner that could be the difference between life and death.
-
@spacesailor: 250 milligrams! Minaturisation continues!!!! The fact you hae A,B,C and D makes me very worried (think hermes)...
-
@WayneL - Soeak for yourself.. I had no idea... Tell us all... How exactly did you know?
-
OK @turboplanner - Let's not get too sensationalistic about it.. the above is why I will never spend money with the Herald Sun (though Robbo on footy is OK). A more seasoned review is here: NFPs face penalty of up to $16.5m or 20 years in prison for directors under new “industrial manslaughter” laws | Lexology. OK, they are talking about not for profits (NFPs), but it is about any workplace death that results from an employer's negligence, which, as the article states, is where standards far well short of those required. I worked for a state H&SE and I have to say, what I saw in my relatively short time was eye opening. The mum and dad businesses that had a minor infraction paid the price; but trying to get a corporate and the directors responsible to be held accountable was impossible. Personally, as described by lexology, I welcome the law - p[particularly the personal liability (although I will say, it should have to be found that it was a direct resuilt of the director's actions or inactions with regard to their responsiilities that they will be held accountable - if it can be shown, for example that they ordered the requisite protection and were misrepresented by their subordinates that it was implemented when it wasn't, then they should not be held liable).
-
Well, the trend these days in minaturisation!
-
So do you know the answer - 50 tons of Canaries
Jerry_Atrick replied to SSCBD's topic in AUS/NZ General Discussion
And only when she is having a cuppa tea.. with two sugars... -
I echo @octave's response above, but as this was addressed to me, I thought I would add one more thing... The assertion is that everything is way over the top and the "mathematically illiterate" are gullible and there is something that experts - people with decades of experience in medicine consulting with people with decades of experience with outbreaks, don't know that is known by others. Yet, no credible evidence has been proffered. Without validating the data sources, I googled Japan covid cases (japan covid cases - Google Search) and Australia Covid Cases (australian covid cases - Google Search) One of the assertions is that it only really badly affects areas with high population densities. Well, take a look at the Japanese numbers.. By any valid comparison, a population density of at least 10 times Australia*, yet their peak number of cases in their second wave is not even twice the number of that in Australia - and given most have occurred in Northern outer parts of Melbourne, I would guess that the relative population densities are quite a bit less than a factor of 10 (as an aside, ACT has a pretty hefty population density of over 1,000/sq mile). They don't precisely correlate in a linear way and I am not going to see if there is any other correlation. The thing is, the vast majority of the numbers in Australia (I have not checked Japan) originate from specific areas; probably from specific events** (BLM, work places and horny security guards come to mind); I guess it's too cold to flock to the beaches). I am all for reasonable and proportional restrictions to the risk; my concern is that the phrase "reasonable and proportional" especially combined with, "for the mathematically illiterate" is a vehicle to unilaterally water down the restrictions without true regard for the risk. At present, we know the fatality rate, but what we don't have ready figures for are the rates of chronic impairment distributed over different levels of severity so we can measure life changing chronic impairment. Also, key is the transmission rate ® and reducing it (I think that is as plain as the nose on my masked face). We know it's behaviour is exponential (as with many contafgeous diseaeses). We know it has a long incubation period so working out you have it before taking precautions once you notice you have symptoms to avoid transmission is futile. Unlike HIV, which is realtively hard to spread without being in close contact and transmission of body fluids - and even then, unless there is direct transmission into the bloodstream, even a set of inhibitor (anti-viral) drugs would be a very expensive exercise as a signfiicant proportion of the population would contract it.. While I accept if I am promiscuous and have unprotected sex with every man, woman and chimp that consents I may end up having to take and anti-viral for the rest of my life, I can elect to wear a condom and drastically reduce the chances. Now, wearing a condom is sort of like wearing a mask at the end of the day.. it does reduce enjoymnent, but it serves to reduce transmission. Yet no-one sees wearing a condom as a violation of their human rights... Of course they have a choice, but I am sure, if it were enforceable, law makers would have loved to, in the days prior to the anti-virals, have a law preventing unprotected sex except when intending to procreate.. but enforcing it is not practical - and HIV doesn't have the transmission rate of COVID. On the other hand, enforceing restrictions is more pragmatic and it does have a wild transmission rate. My point.. the lockdown is to get ahead of an exponential increasining of transmissions - look at the curves of the two graphs - even mathematically illiterate can see the patterns. IMHO, they show how it can quickly get out of control; Once under control, social distancing, masks, etc, is required to keep it there. It sort of makes sense. Yes, I take the point it provides other pain and suffering.. the question is of scale.. I am lucky, I live in a big (although renovators delight) house in a village on a decent plot of land outside of London. I feel very sorry for those families in a small flat in a tower block (as I do for those in housing commissions in Melbourne). We should be providing them support and relief - that is sympathetic to their cultures e.g. special dietary requierements, maybe some timetable of exercise out of the house, financial support, medicines, pastoral care, etc. I absolutely agree... But, the maths speak for themselves so far, to this illiterate person. * You could also find areas in Japan on a par of population density or even less than areas in Australia. But like for like, relative to the country (e.g. captial cities, etc), it does appear to be that. Of course, Tokyo is only 6 times more populated that ACT, so I compared it to Sydney which was actually way more than 10 times... I compared Sydney to Okinawa, which gave more than twice the population density, however, that is like comparing Sydney to Geelong, maybe. It appears going hard has results regardless of population density (but, if you live in an area of 3 people per square mile, then going hard is not coming within 100' of your neighbour). ** I don't know what caused the outbreaks in Melb - just potential causes... so happy to be corrected.. .Well, happy to be corrected with any of the above. [edit] Looking at US Stats (google COVID-19 Cases USA), where it can be argued they have let it to a certain extent rip, their fatality rate is 3.5% - almost 3.5 times ours..They have a similar health system (although poublic health is not as good as ours), but that doesn't account for the massiv difference in fatality rates. Note, the global reported fatality rate is 3.9% and that includes many countries without developed public health facilities. That should provide some food for thought. Also, lool at their curve - more or less plateaued during their controversial period of lockdowns and restrictions; but as they have eased, well... the data is there...
-
Hi @SplitS, Can you please educate us mathematically illiterate, using credible sources, where the official maths is wrong? After all, stating "for the mathematically illiterate" is all well and good, but without real cedible evidence, it is a hollow claim. I know and understand that the death rate is c 1% of reported cases (and it appears that increasing the testing correlates to an increased identification in number of infections, but given the concern of the number of increased deaths attributed to pnuemonia, there is a concern there is also an underreporting of deaths as well). I also know that the death rate is lower amongst the younger population, but it seems to be catching out a number of people with hitherto unknown conditions susceptible to becoming a fatality under COVID-19 who were living normal, active lives. We also know the spread is exponential and has the propensity to overwhelm the health services because of the extra-long incubation period before symptoms are exhibited and that a relatively high population will require hosptialisation to the point where hospitals will have to turn people away. Intuitiviely, in such a scenario where people are being turned away from necessary hosptial treatment, (and as witnessed in NYC), the death rate will increase as a result. I haven't done the research and to be honest, I can't be bothered because I trust our health officials.. so far they have not been materially wrong unless everything we are being told and the stats that are being kept is complete BS. In this situation, it is hard to be statisctically precise to the individual case, but all the maths and stats I have seen do not paint a rosy picture to just let it rip - even protecting the known people with pre-existing conditions and the elderly.... The medical profession may be erring on the side of caution, but in this case, so far, the evidence has borne out support of this approach rather than throwing caution to the wind. But let's go the other way... Let's isolate a decent sized part of the population representative of the greater population at large, including proprotional sized health facilities, age ranges, known pre-conditions and we can assume unknown pre-conditions; and, of course, thrown in a proprtional number of people estimated to have the virus today ... let the virus rip and see what happens. Will you volunteer to be in that test? I certainly wouldn't - nor would I allow any of my family - and I would strongly dissuade anyone else.